
Starting date: July 2021
Work Programme
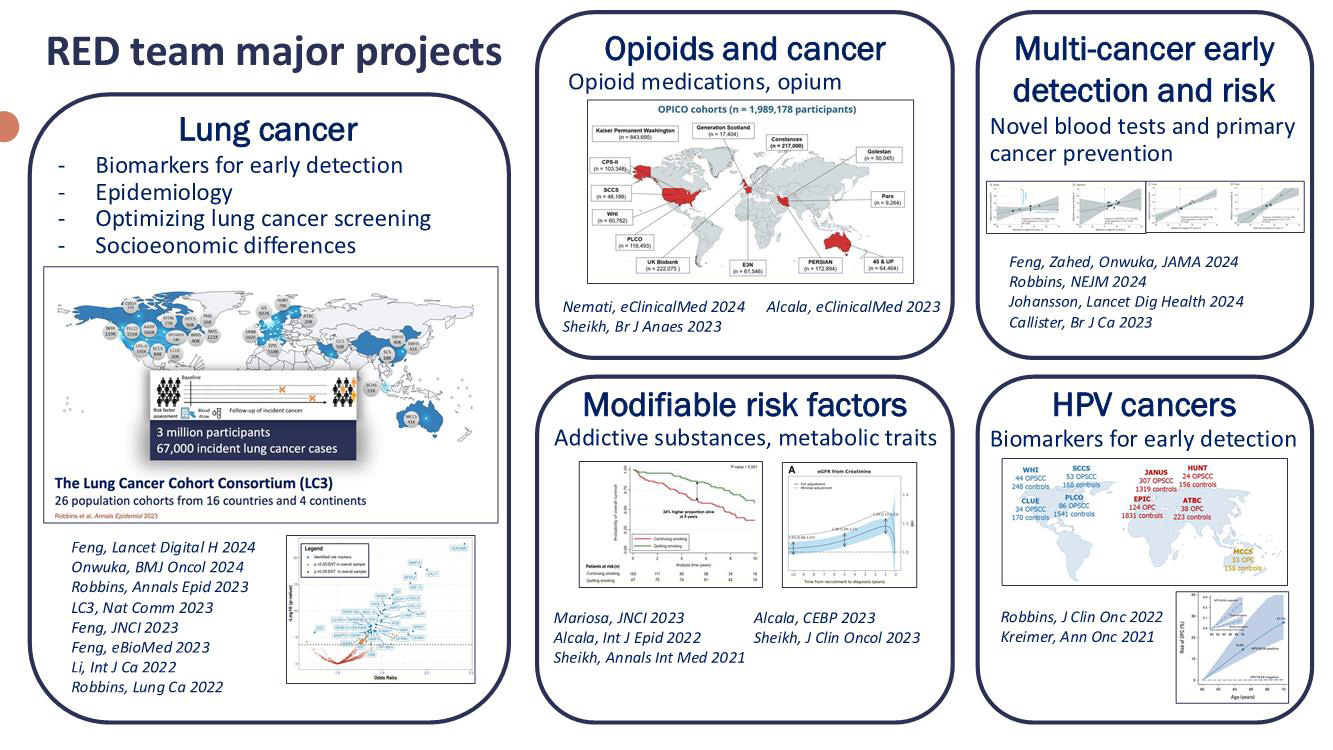
The Risk Assessment and Early Detection Team (RED) carries out translational epidemiological research spanning from discovery to implementation. RED’s ambition is to lead research with strong potential for long-term impact in reducing the impact of cancer.
The vision of RED is:- to inform primary prevention by advancing the understanding of cancer risk and etiology; and
- to inform secondary prevention by optimizing early detection strategies.
RED specializes in organizing large international collaborations to study risk factors, develop risk prediction tools, and identify and evaluate early detection biomarkers. RED leverages the specific strengths of different conceptual, design, and analytical approaches to reach conclusive answers to important research questions, often leveraging the rich data resources generated by consortium studies.
A specific objective is to evaluate the importance of evolving risk factors in cancer etiology among populations in transition, including opioid and tobacco use and obesity. RED approaches this by organizing collaborative projects with investigators around the world to measure risk factors directly using traditional observational methods, and using instrumental variable methods by leveraging large genomic studies.
Another objective is to develop methods for improved early detection of cancer. A key strategy in this field is to improve cancer-specific risk assessment by incorporating novel risk indicators, frequently biomarkers, and to validate existing risk prediction tools in diverse populations. A guiding principle is to design studies that mimic the target use population to directly motivate implementation studies of biomarkers for early cancer detection.
RED focuses on several cancer types, with a particular emphasis on lung cancer, kidney cancer, and human papillomavirus (HPV)-associated cancers. All RED projects involve international collaborations, and many include the coordination of large consortia.
Team Composition
Team Leaders: Dr Mattias Johansson and Dr Hilary Robbins, Genomic Epidemiology Branch (GEM), IARC
Emails: JohanssonM@iarc.who.int; RobbinsH@iarc.who.int
Team members:
Dr Mahdi Sheikh (Scientist, GEM)
Dr Xiaoshuang Feng (Scientist, GEM)
Dr Shaymaa Alwaheidi (Project Officer, GEM)
Ms Karine Alcala (Senior Research Assistant, Data Management/Analysis, GEM)
Ms Andreea Spanu (Project Assistant, GEM)
Dr Allison Domingues (Postdoctoral Scientist, GEM)
Dr Hana Zahed (Postdoctoral Scientist, GEM)
Dr Justina Onwuka (Postdoctoral Scientist, GEM)
Dr Ryan Langdon (Postdoctoral Scientist, GEM)
Dr Jia Liu (Visiting Scientist, GEM)
Dr Jifang Zhou (Visiting Scientist, GEM)
Dr Saeed Nemati (Visiting Scientist, GEM)
Mr Aghiles Guenoun (Master’s Student, GEM)
Ms Marie-Pierre Nobels (Master’s Student, GEM)
Key networks: Lung Cancer Cohort Consortium (LC3), International Lung Cancer Consortium (ILCCO), MetKid Consortium, Integrative Cancer Epidemiology Programme (ICEP), HPV Cancer Cohort Consortium (HPVC3), Opioid Cohort Consortium (OPICO)
Key funding: United States National Cancer Institute (NCI), World Cancer Research Fund (WCRF), Lung Cancer Research Foundation (LCRF), Institut national du Cancer (INCa), Cancer Research UK (CRUK)
Key publications
- Feng X, Zahed H, Onwuka J, Callister MEJ, Johansson M, Etzioni R, et al. (2024). Cancer stage compared with mortality as end points in randomized clinical trials of cancer screening: a systematic review and meta-analysis. JAMA. 331(22):1910–7. https://doi.org/10.1001/jama.2024.5814 PMID:38583868
- Feng X, Goodley P, Alcala K, Guida F, Kaaks R, Vermeulen R, et al. (2024). Evaluation of risk prediction models to select lung cancer screening participants in Europe: a prospective cohort consortium analysis. Lancet Digit Health. 6(9):e614–24. https://doi.org/10.1016/S2589-7500(24)00123-7 PMID:39179310
- Alcala K, Poustchi H, Viallon V, Islami F, Pourshams A, Sadjadi A, et al. (2023). Incident cancers attributable to using opium and smoking cigarettes in the Golestan Cohort Study. EClinicalMedicine. 64(64):102229. https://doi.org/10.1016/j.eclinm.2023.102229 PMID:37781157
- Albanes D, Alcala K, Alcala N, Amos CI, Arslan AA, Bassett JK, et al.; Lung Cancer Cohort Consortium (LC3) (2023). The blood proteome of imminent lung cancer diagnosis. Nat Commun. 14(1):3042. https://doi.org/10.1038/s41467-023-37979-8 PMID:37264016
- Feng X, Wu WYY, Onwuka JU, Haider Z, Alcala K, Smith-Byrne K, et al. (2023). Lung cancer risk discrimination of prediagnostic proteomics measurements compared with existing prediction tools. J Natl Cancer Inst. 115(9):1050–9. https://doi.org/10.1093/jnci/djad071 PMID:37260165
- Sheikh M, Mukeriya A, Zahed H, Feng X, Robbins HA, Shangina O, et al. (2023). Smoking cessation after diagnosis of kidney cancer is associated with reduced risk of mortality and cancer progression: a prospective cohort study. J Clin Oncol. 41(15):2747–55. https://doi.org/10.1200/JCO.22.02472 PMID:36989465
- Robbins HA, Ferreiro-Iglesias A, Waterboer T, Brenner N, Nygard M, Bender N, et al. (2022). Absolute risk of oropharyngeal cancer after an HPV16-E6 serology test and potential implications for screening: results from the Human Papillomavirus Cancer Cohort Consortium. J Clin Oncol. 40(31):3613–22. https://doi.org/10.1200/JCO.21.01785 PMID:35700419
- Zahed H, Feng X, Sheikh M, Bray F, Ferlay J, Ginsburg O, et al. (2024). Age at diagnosis for lung, colon, breast and prostate cancers: an international comparative study. Int J Cancer. 154(1):28–40. https://doi.org/10.1002/ijc.34671 PMID:37615573
- Alcala K, Zahed H, Cortez Cardoso Penha R, Alcala N, Robbins HA, Smith-Byrne K, et al. (2023). Kidney function and risk of renal cell carcinoma. Cancer Epidemiol Biomarkers Prev. 32(11):1644–50. https://doi.org/10.1158/1055-9965.EPI-23-0558 PMID:37668600
- Kachuri L, Graff RE, Smith-Byrne K, Meyers TJ, Rashkin SR, Ziv E, et al. (2020). Pan-cancer analysis demonstrates that integrating polygenic risk scores with modifiable risk factors improves risk prediction. Nat Commun. 11(1):6084. https://doi.org/10.1038/s41467-020-19600-4 PMID:33247094