Household fuel use and the risk of gastrointestinal cancers: the Golestan Cohort Study
A new study published today in the journal Environmental Health Perspectives provides strong evidence that household burning of biomass and kerosene fuels, especially using stoves without a chimney, increases the risk of developing several cancers of the digestive tract.Indoor burning of biomass and kerosene fuel Press Release
IARC Press Release 285
Indoor burning of biomass and kerosene fuels is associated with higher risk of developing several types of digestive cancersDownload PDF
Questions and Answers
Questions and Answers

1. Can you tell us a bit more about the study and its methodology?
It is well documented that the combustion of non-clean fuels, including coal, biomass, and kerosene, produces multiple carcinogenic compounds. There is a large body of evidence showing that exposure to the emissions from coal combustion can increase the risk of lung cancer in humans, which resulted in this exposure being categorized by the IARC Monographs programme as “carcinogenic to humans” (Group 1). However, despite the widespread use of biomass and kerosene fuels, involving almost 40% of the world’s population, there is still inadequate information on these exposures and their carcinogenicity.
Given the evidence showing that carcinogenic compounds resulting from the combustion of non-clean fuels can be absorbed through the digestive tract, and the fact that the burden of digestive cancers is higher in areas where exposure to household fuel combustion emissions is highest, a thorough assessment of these exposures and their effects on the risk of digestive cancers was necessary. The Golestan Cohort Study provided a unique opportunity to investigate this hypothesis, because of its large sample size, its location in a region with high rates of digestive cancers, its enrolment of a mostly rural population that uses kerosene and biomass fuels for household purposes, and limited confounding effects from alcohol consumption and smoking, due to low consumption rates in the participants (especially in women).
The Golestan Cohort Study is a population-based prospective cohort study of individuals aged 40–75 years residing in Golestan Province in north-eastern Islamic Republic of Iran. The Golestan Cohort Study was initiated in 2004 by the Digestive Disease Research Institute of the Tehran University of Medical Sciences, in collaboration with the International Agency for Research on Cancer (IARC) and the United States National Cancer Institute. During the enrolment phase of the project, which lasted for 4 years until 2008, detailed data were collected on demographics, socioeconomic status, lifestyle, household fuel use, type of heating stove, and various other exposures. In addition, responses to a detailed food frequency questionnaire were collected, and a biobank was built that included samples of blood, urine, hair, and nails from all participants. Since the enrolment, more than 99% of the participants have been successfully followed up through annual telephone surveys and home visits (in the case of a reported death or incident cancer). Furthermore, all cancer cases are matched to the Golestan Population-based Cancer Registry, which is a high-quality cancer registry that was also initiated in collaboration with IARC, in 2001.
The current study is based on analysing the data on lifetime use of household fuels from more than 50 000 participants in the Golestan Cohort Study who have been followed up for more than 10 years.
2. Who is more at risk?
According to estimates from the World Health Organization (WHO), about 3 billion people worldwide still heat their homes and cook using solid fuels (such as wood, crop wastes, charcoal, coal, and dung) and kerosene in open fires and inefficient stoves. Most of these people are poor and live in low- and middle-income countries. Exposure is particularly high among women and young children, who spend the most time near the domestic hearth.
Based on IARC Monographs Volume 95, exposure to indoor air pollutants that are associated with the combustion of solid fuels for cooking and heating is extensive in South Asia; this exposure is widespread and prevalent in one half to three quarters of the population in most countries in that region. In Latin America, nearly 25% of the population live in rural areas, where biomass fuels are most frequently used for cooking and heating. In Africa, biomass fuel is used almost exclusively in rural areas and is still widely used in most urban areas.
3. What do the results of this study show?
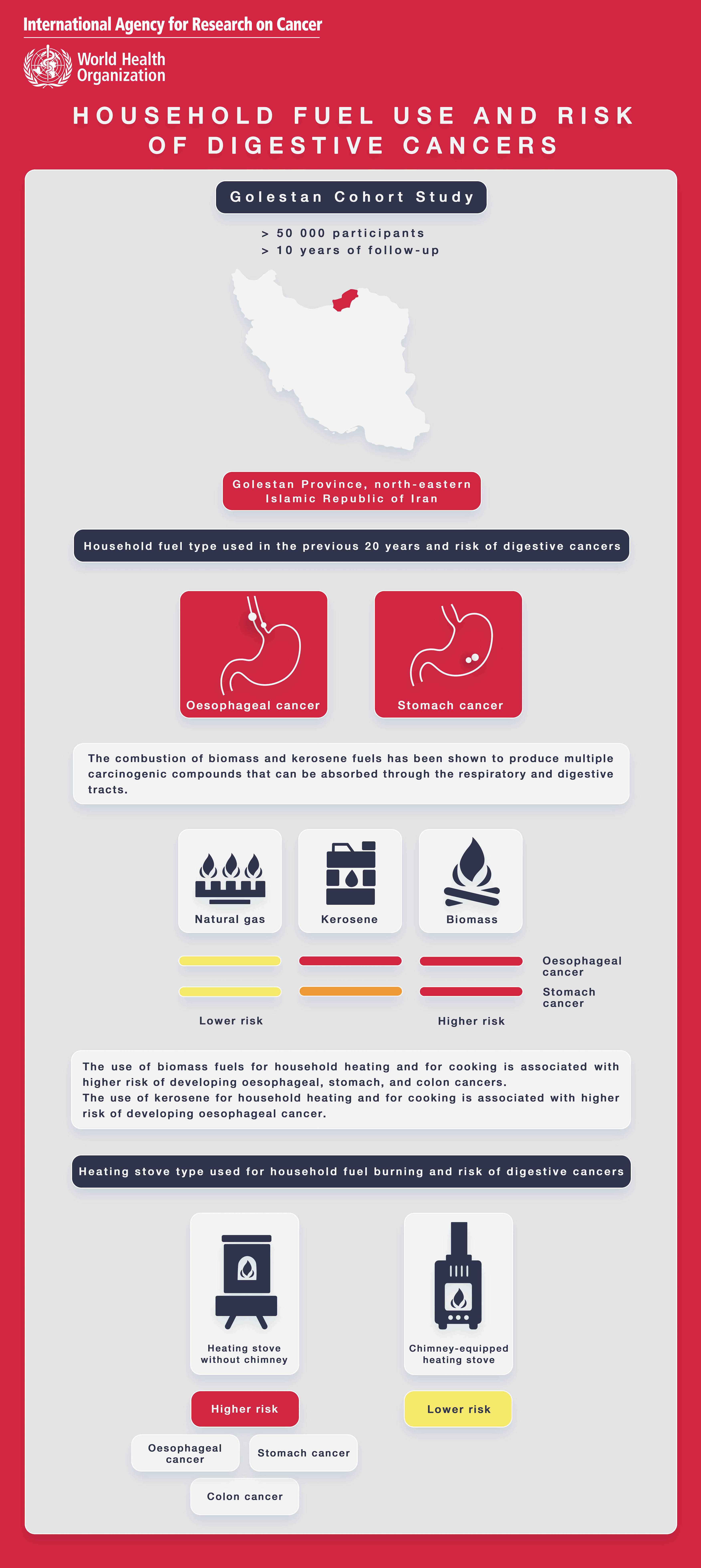
In the current study, higher risks of oesophageal, gastric, and colon cancers were observed in participants who burned biomass for home heating and cooking. The risk was notably high when the participants reported burning biomass fuels using heating stoves without a chimney, and the risk was significantly lower when biomass was burned using chimney-equipped heating stoves.
This study also showed a higher risk of oesophageal cancer in participants who burned kerosene for cooking and for home heating, and the risk was also significantly higher when this fuel was burned using heating stoves without a chimney compared with using chimney-equipped heating stoves.
We did not observe meaningful associations between use of fuels and risk of pancreatic cancer or liver cancer.
In summary, this study shows that household burning of biomass and kerosene, especially using a stove without a chimney, may increase risk of some cancers of the digestive system.
4. What is new in this study?
We knew that combustion of these fuels produces multiple carcinogenic compounds that can be absorbed through the respiratory and digestive tracts. Our knowledge about the cancer risk associated with using these fuels in humans originates mostly from retrospective studies with a limited number of participants, which had focused on respiratory cancers, whereas the risk among the exposed individuals of developing other cancer types, including digestive cancers, has been largely understudied.
This study provides the first evidence from a large population-based prospective cohort study on the possible carcinogenic effects of household burning of biomass and kerosene fuels in humans. This study also provides strong evidence that the increased cancer risk among individuals who are exposed to the indoor combustion of biomass and kerosene fuels may extend beyond the respiratory system and affect several sites of the gastrointestinal tract.
Another important finding in this study was that using chimney-equipped stoves while burning biomass or kerosene fuels was associated with lower risk of digestive cancers compared with burning the same fuels using stoves without a chimney. This finding could have a great impact on public health and policy-making in the affected regions.
5. What are the mechanisms at play that increase these risks?
The exact mechanisms are still not known. However, one possible mechanism might be through the local and systemic exposure of the digestive organs to the carcinogenic compounds that are present in the emissions from combustion of solid fuels and kerosene; these compounds include polycyclic aromatic hydrocarbons (PAHs), benzene, and formaldehyde. Higher exposure to emissions from combustion of biomass fuels may increase the systemic absorption of these carcinogenic compounds through the respiratory and digestive tracts, as documented in studies that have demonstrated high urinary levels of PAH metabolites, benzene, and carbon monoxide in individuals who were using biomass fuels, and studies that showed reduced urinary levels of PAH metabolites after interventions with improved chimney-equipped stoves. There is accumulating evidence that suggests a possible role for PAHs in the pathogenesis of digestive cancers, including studies that showed high levels of PAH biomarkers in the urine or oesophageal tissues of patients with oesophageal cancer and in rectal tissues of patients with rectal cancer. This hypothesis is further supported by studies that have shown higher levels of PAH–DNA adducts in patients with gastric, colorectal, and oesophageal cancers.
6. How significant is the risk of developing these cancers?
When we compared the risk of digestive cancers among the participants based on the type of fuels that they had predominantly used for household purposes in the previous 20 years, we found an almost 90% higher risk of developing oesophageal cancer in participants who used mainly biomass and those who used mainly kerosene, compared with participants who used mainly natural gas for household purposes. We also found an about 80% higher risk of developing gastric cancer in participants who used mainly biomass, compared with those who used mainly natural gas for household purposes. A higher risk of developing colon cancer was observed only when biomass was burned using heating stoves without a chimney; this was an increase of 25% in the risk of colon cancer with every 10 years of burning biomass using heating stoves without a chimney.
7. What is the WHO position on household burning of biomass and kerosene?
According to WHO estimates, about 3.8 million people per year die prematurely from illness attributable to the household air pollution caused by the inefficient use of solid fuels and kerosene for cooking. Without a substantial policy change, the total number of people lacking access to clean fuels and technologies will remain largely unchanged by 2030, and this will hinder the achievement of the United Nations 2030 Agenda for Sustainable Development.
To ensure healthy air in and around the home, WHO has released guidelines for indoor air quality and household fuel combustion, which provide health-based recommendations on the types of fuels and technologies to protect health as well as strategies for the effective dissemination and adoption of such home energy technologies. In these guidelines, WHO recommends the prioritization of the transition to technologies and fuels that meet the WHO air quality guidelines. For household fuels, WHO recommends against the use of biomass and unprocessed coal and discourages the use of kerosene.
WHO has also been closely monitoring the evidence on the carcinogenicity of the use of biomass and kerosene fuels, evaluated through the IARC Monographs programme. In IARC Monographs Volume 95, published in 2010, the evidence on the carcinogenic hazards to humans from household use of solid fuels was evaluated by an international Working Group. It was concluded that indoor emissions from household combustion of biomass fuel (primarily wood) are “probably carcinogenic to humans” (Group 2A). At that time, only a limited number of studies in humans were available on this topic, and therefore there was not enough evidence on the cancer hazard from human studies. Since then, several studies have been published in different regions, which resulted in the assignment of a high priority for the re-evaluation of the evidence and the reclassification of the combustion of biomass fuels by the IARC Monographs programme within the next 3 years.
The carcinogenic hazards to humans from kerosene were evaluated in IARC Monographs Volume 45, published in 1989. The Working Group concluded that there is limited evidence for the carcinogenicity in experimental animals of straight-run kerosene. Also, there were no human studies evaluating this risk. There has been little progress in this field, and very few human studies have aimed to evaluate the cancer risk related to the combustion of kerosene.
Due to the paucity of relevant studies, WHO recently called for further research into the health impacts of kerosene.
8. How can people protect themselves from this risk?
The best way is to replace these non-clean fuels with clean fuels (including natural gas, electricity, and solar cookers). If this is not achievable, replacing the traditional inefficient stoves with newer chimney-equipped stoves and also proper home ventilation might be appropriate for lowering the health hazards associated with using non-clean fuels.
9. What do you expect from these results?
These results provide new evidence on the cancer risk associated with long-term use of biomass and kerosene fuels and should therefore help to shape efficient public health policies to protect the populations most at risk.
Infographic